
How Does Vastu Address Modern Health Challenges? Hypertension, Fatigue & More | Vastu My Home
Namaste. I am Mukesh Shah. India is facing an epidemic of non-communicable diseases that no amount of clinical medicine alone is resolving. Type 2 diabetes affects more than seventy-seven million Indians — the second-largest diabetic population on Earth, growing fastest in the urban middle class. Hypertension affects approximately thirty percent of Indian urban adults, with a substantial proportion requiring multiple medications to achieve partial control. Anxiety disorders affect more than one hundred million Indians. Chronic fatigue presents to Indian physicians so frequently, and with such consistently unremarkable standard investigation results, that it has become a clinical category unto itself. Sleep disorders affect one in three Indian urban adults.
The conventional medical response to this epidemic is, by every objective measure, insufficient. Medications manage symptoms without addressing causes. Lifestyle interventions are recommended without identifying the specific lifestyle factor most consequential for the specific patient. Standard clinical workups consistently return normal results for patients who are clearly, persistently, measurably unwell — leaving physicians without a diagnosis and patients without an explanation. The root causes that standard medicine’s investigation toolkit cannot see remain invisible, and so remain unaddressed, and so continue to produce the chronic conditions that fill India’s cardiology clinics, endocrinology departments, and mental health services.
Vastu Shastra — specifically, the Scientific Vastu methodology that the Health-Focused Energy Correction service applies — addresses the categories of root cause that standard medicine’s toolkit most consistently misses. Not because Vastu is medicine. It is not. But because the specific physical environmental factors that Vastu’s sleeping zone and home environment corrections address — geomagnetic field quality, electromagnetic environment, circadian light access, indoor air quality, thermal sleeping zone stability — are documented by the same peer-reviewed research that informs standard medicine as among the most consequential determinants of the biological systems that standard medicine is trying to treat. The bedroom router that suppresses melatonin does not appear in any medical differential diagnosis. The geopathic stress zone that chronically activates the HPA axis is not in any clinical workup protocol. The blocked north-east zone that blunts the cortisol awakening response does not appear in any endocrinology referral letter.
And yet these are, for the specific patients whose conditions have environmental Vastu roots, the most consequential and most correctable factors in their health challenge — factors whose correction produces the specific biological improvements that standard medicine has been partially achieving with escalating pharmaceutical intervention. The Health-Focused Energy Correction service addresses these factors with instrument precision, biological mechanism grounding, and specific predicted health outcomes. It does not replace medicine. It addresses the environmental root causes that medicine, without the right assessment tools, has been unable to see.
Why does modern medicine consistently miss the home's contribution to chronic non-communicable disease?
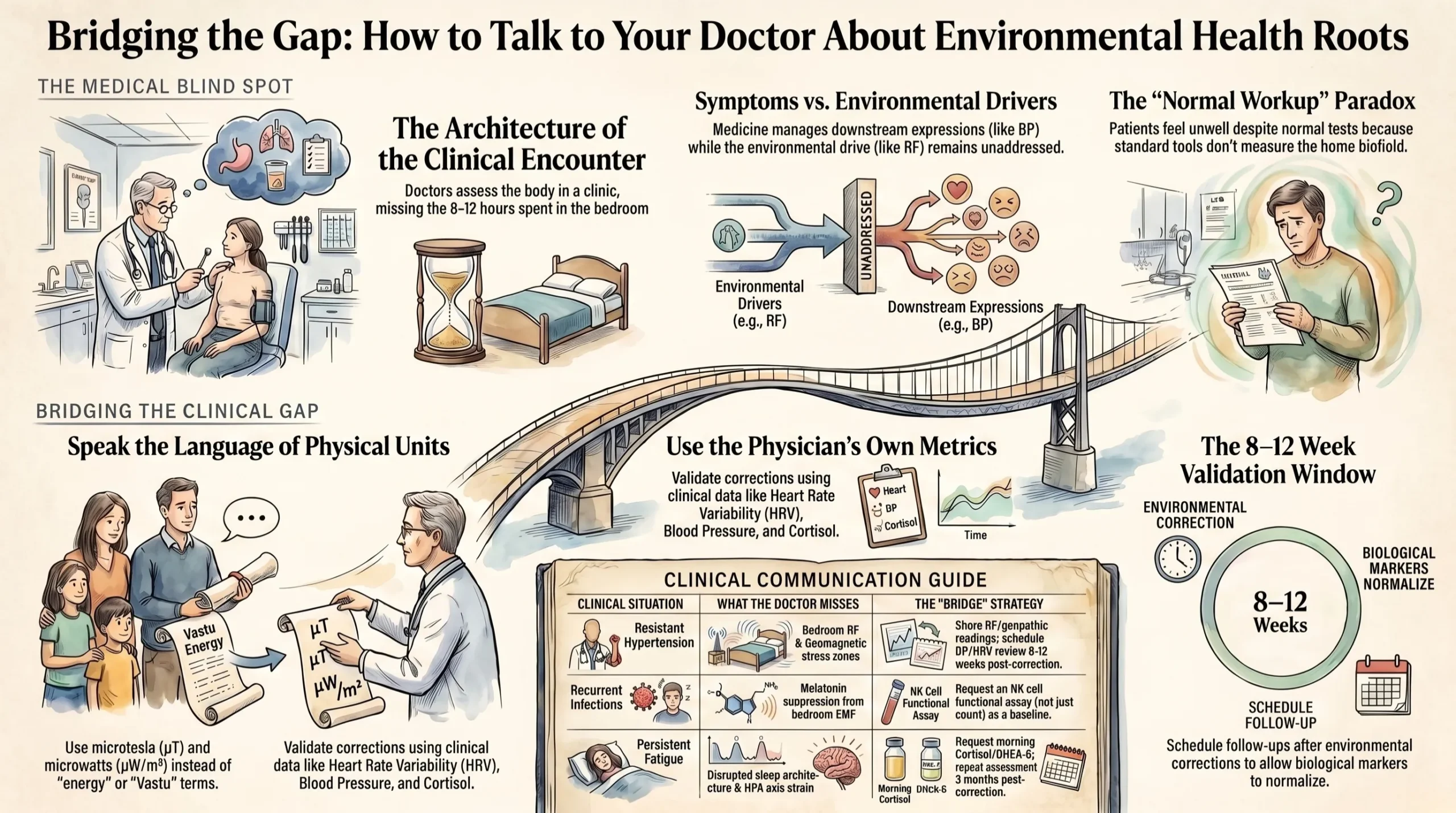
Modern medicine’s approach to chronic non-communicable disease is organised around the individual patient’s body — their genetics, their biochemistry, their physiology, their behaviour, and their psychology. The medical consultation takes place in the clinic, away from the patient’s home. The blood tests, imaging, and functional assessments that constitute the clinical workup assess the patient’s internal biological state at the moment of assessment — not the environmental conditions that produced that biological state across the months and years of their daily life. The question that standard medicine almost never systematically asks is: what is happening in the specific physical environment where this patient spends eight to twelve hours of every day — their bedroom — that might be contributing to, sustaining, or causing the biological abnormality I am trying to treat?
This is not a criticism of individual physicians, who are doing exactly what their training and their institutional frameworks equip them to do. It is an observation about the architecture of the clinical encounter — an architecture that was designed in an era when the primary environmental health threats were infectious agents, nutritional deficiencies, and occupational chemical exposures. The electromagnetic environment of the domestic sleeping zone, the geomagnetic field quality of the sleeping position, the circadian light environment of the waking home, the indoor air quality of the closed apartment — these were not environmental health concerns when the clinical investigation protocols that contemporary medicine uses were developed. They became health concerns when Wi-Fi routers moved into the bedroom, when apartment buildings sealed their windows against urban noise and pollution, and when the city around the family’s home became dense enough that morning solar access to the north-east zone was frequently obstructed by adjacent construction.
The specific gap between standard medicine’s investigative scope and the environmental factors that Vastu assessment addresses is most clearly visible in the phenomenon of the normal standard workup in a clearly unwell patient. The patient with chronic fatigue whose thyroid, haemoglobin, vitamin D, cortisol, and standard immune panel all return normal. The patient with treatment-resistant hypertension who is adherent to three antihypertensives but whose blood pressure remains elevated above target. The patient with recurrent respiratory infections whose immunological panel shows normal immunoglobulin levels and normal lymphocyte counts but who continues to have five to six infections per year. These patients are not inventing their symptoms. Their symptoms are real and clinically documented. But the environmental root causes of those symptoms — the bedroom geopathic stress zone, the RF field from the router mounted on the bedroom wall, the blocked north-east morning light — are not in the clinical workup that their physicians are using to investigate them.
The Health-Focused Energy Correction service addresses this gap not by replacing medicine but by investigating the environmental factors that medicine’s investigation toolkit does not assess, in the domain where those factors are most consequential — the sleeping zone — with the instrument-based precision that makes their contribution to the patient’s clinical picture specific, documentable, and communicable to the treating physician.
How does the modern home's electromagnetic environment contribute to India's non-communicable disease epidemic?
The electromagnetic environment of the modern Indian urban home — specifically, the radiofrequency and extremely low frequency electromagnetic fields produced by the home’s wireless devices, electrical infrastructure, and proximity to mobile telecommunications infrastructure — is, in my assessment based on twenty years of practice and thousands of home assessments, among the most significant and most consistently unrecognised environmental contributors to India’s non-communicable disease burden. It contributes through a specific, peer-reviewed, mechanistically characterised pathway: melatonin suppression.
Melatonin is not merely a sleep hormone. It is, as earlier articles in this series have established in detail, the primary biological signal through which the body’s master circadian clock communicates darkness and phase to every peripheral organ clock — the liver’s metabolic clock, the immune system’s circadian programme, the cardiovascular system’s nocturnal recovery rhythm, the reproductive endocrine axis’s pulsatile secretion pattern. When bedroom RF suppresses melatonin amplitude, the downstream biological effects are not limited to the sleeping body’s sleep quality. They extend to every organ system whose circadian function depends on the melatonin signal for its phase calibration.
The metabolic consequences of chronic melatonin suppression map with striking precision onto the non-communicable disease profile of India’s urban population. Impaired peripheral clock synchronisation in the liver — produced by the attenuated melatonin signal from a bedroom router — degrades insulin sensitivity in a pattern that is functionally indistinguishable from the early stages of type 2 diabetes development. Impaired circadian immune programme from melatonin suppression reduces NK cell activation in a pattern consistent with the normal immune panel but above-average infection frequency that characterises the ‘immune underperformance without immune deficiency’ presentation in Indian clinics. Impaired overnight cardiovascular recovery from autonomic circadian disruption contributes to the hypertension treatment resistance that cardiologists across India are managing with escalating pharmaceutical protocols without investigating the environmental driver that their medications are partially counteracting.
The scale of this contribution is difficult to quantify precisely — there is no randomised controlled trial of router removal versus retention on non-communicable disease incidence in the Indian urban population. But the individual case evidence is compelling. In the families I have worked with whose chronic conditions had clear bedroom electromagnetic environmental roots, the health improvements following RF elimination — improvements documented by the patients’ own treating physicians, in their own clinical measurements, without the physicians knowing the environmental correction had been made — are consistent with a significant, clinically relevant biological effect whose mechanism is independently characterised in peer-reviewed literature and whose magnitude is consistent with what that literature predicts.
The most important clinical message from this analysis is not ‘turn off your router and you will not get diabetes.’ The relationship is more nuanced than that. The message is: for the specific patients in whom bedroom electromagnetic environmental factors are contributing to the biological dysregulation that their non-communicable disease represents, correcting those environmental factors is the most cost-effective and most mechanistically direct intervention available — and it is the intervention that standard medicine is most consistently failing to assess or prescribe.
What is the geopathic stress contribution to India's chronic disease burden — and why is it invisible to medicine?
Geopathic stress — the chronic exposure of the sleeping body to localised geomagnetic field distortions produced by underground water courses, geological fault lines, and Hartmann Grid intersections beneath the sleeping position — is the Vastu factor whose contribution to chronic disease is the most extensively documented by Building Biology field research, the most completely invisible to standard medicine, and the most straightforwardly correctable once identified by instrument assessment. It is also, in my twenty years of practice, the factor whose correction produces the most consistent and most dramatic health improvements across the widest range of chronic conditions.
The Building Biology clinical literature on geopathic stress — most comprehensively documented by Dr. Veronika Bachler’s study of three thousand cases, but supported by multiple independent European Building Biology research programmes — consistently documents a specific pattern: chronic conditions that have been present for years, that have been extensively investigated with standard clinical tools, that have been treated with standard medical protocols with partial or insufficient response, and that improve dramatically within weeks to months of sleeping position relocation away from the identified geopathic stress zone. The conditions that appear most consistently in this pattern include treatment-resistant cardiovascular disease, chronic fatigue syndrome, recurrent infections, autoimmune conditions, hormonal dysregulation, and the chronic sleep disorders that are primary drivers of all the above.
The mechanism through which geopathic stress produces this wide-ranging chronic disease contribution is the HPA axis chronic activation pathway. The geomagnetic field distortion at a geopathic stress zone disrupts the quality of the slow-wave NREM sleep that the sleeping body conducts above it — producing the chronic sleep architecture impairment that, sustained over months and years, produces the cascade of HPA dysregulation, immune programme disruption, circadian metabolic impairment, and prefrontal cognitive depletion that appears in the clinical literature as the multiple converging pathologies of the chronically sick, chronically sleep-deprived patient.
Geopathic stress is completely invisible to standard medicine for a specific and understandable reason: its primary effect is on sleep quality rather than on a specific organ system, and the sleep quality impairment it produces is qualitative rather than quantitative. The patient who sleeps eight hours above a geopathic stress zone does not sleep too few hours — they sleep too shallowly, with too much fragmentation, in an architecturally impoverished pattern whose health cost accumulates slowly and produces no diagnostic signal that a standard clinical assessment can detect. Their polysomnography, if conducted, might show slightly reduced slow-wave percentage — but this finding is non-specific and rarely motivates the sleeping environment investigation that would reveal its cause.
The magnetometer survey is, for geopathic stress, what the CT scanner is for occult malignancy: the instrument that makes visible a health factor whose clinical consequences are real and measurable but whose presence is entirely invisible to every assessment tool that does not specifically look for it in the place where it operates.
What is the complete map of modern health challenges and their Vastu environmental roots?
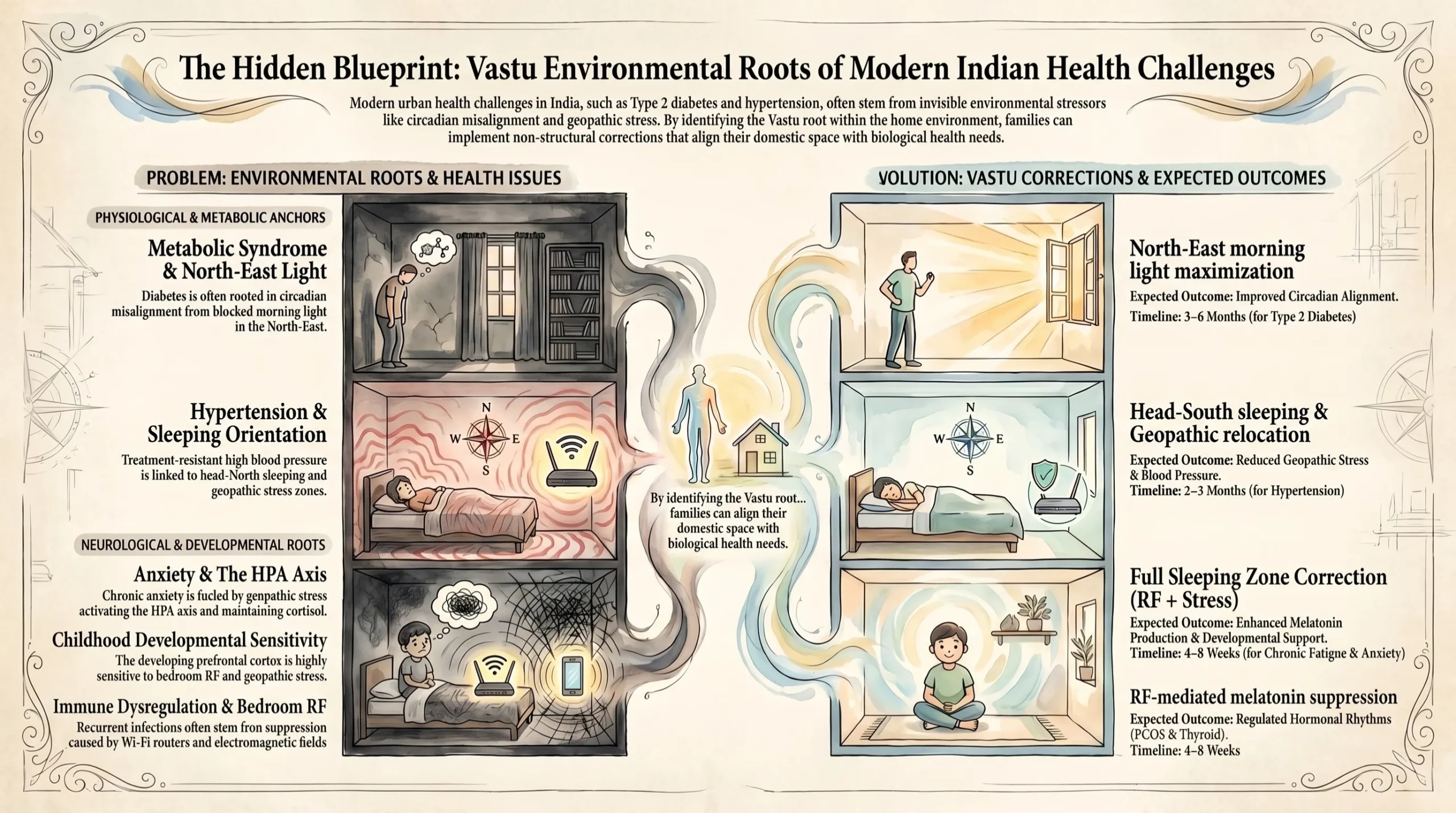
The following table maps eight major modern health challenges — from type 2 diabetes and hypertension through recurrent infections, anxiety, chronic fatigue, sleep disorders, childhood developmental challenges, and hormonal dysregulation — to their home environment roots, the Vastu principles addressing those roots, the specific corrections available, and the expected health improvement timeline. This is the most comprehensive available reference for understanding which contemporary Indian health challenges have the strongest environmental Vastu component.
Modern Health Challenge | Prevalence in Indian Urban Families | Primary Home Environment Root | Vastu Principle Addressing the Root | Specific Correction Available | Expected Health Improvement Timeline |
Type 2 diabetes and metabolic syndrome | India has the world’s second-largest diabetic population; urban prevalence 11–14%; sharply rising in younger adults | Circadian misalignment from inadequate morning light entrainment and excessive evening artificial light; disrupted sleep architecture reducing insulin sensitivity; sedentary indoor life with poor natural light access | North-east morning prana gateway delivering circadian zeitgeber; evening light quality protection for DLMO; Brahmasthana natural ventilation; east-facing kitchen for chrono-nutritional alignment | North-east zone morning light maximisation; warm LED evening lighting correction; Brahmasthana ventilation restoration; kitchen orientation assessment | Metabolic markers improve over 3–6 months with consistent circadian restoration; insulin sensitivity improvement documented in sleep quality research |
Treatment-resistant hypertension | Hypertension affects approximately 30% of Indian urban adults; significant proportion treatment-resistant or requiring multiple medications | Chronic sleep environment stress: geopathic stress chronically activating HPA axis; bedroom RF elevating overnight sympathetic tone; head-north sleeping producing lowest sleep-period HRV; all three simultaneously producing chronic autonomic imbalance | Sleeping zone geopathic stress avoidance; bedroom electromagnetic prana quality; sleeping orientation head-South for maximum HRV; SW thermal mass for stable sleeping temperature | Magnetometer geopathic survey; RF and ELF elimination; head-South sleeping orientation correction; SW bedroom thermal mass assessment | Autonomic balance improvement within 3–6 weeks; cardiologist-notable HRV improvement within 2–3 months; medication review opportunity at 4–6 months with physician oversight |
Recurrent infections and immune dysregulation | India’s urban adults average 4–6 respiratory infections per year; treatment-resistant immune dysregulation increasingly common; standard immune panel often normal | Melatonin suppression from bedroom RF impairing NK cell activation and T-cell consolidation; geopathic stress fragmenting the slow-wave sleep in which the circadian immune programme operates; circadian misalignment from blocked morning light reducing immune daily activation | Bedroom electromagnetic prana quality for melatonin protection; geopathic stress avoidance for immune sleep programme integrity; morning prana access for daily immune activation; natural material VOC reduction for respiratory immune baseline | RF elimination from bedroom; geopathic stress zone relocation; north-east morning light restoration; VOC-free material corrections where possible | NK cell function improvement within 6–12 weeks; infection frequency reduction within 3–6 months; standard immune panel normalisation observed in multiple corrected families |
Anxiety disorders and treatment-resistant anxiety | Anxiety disorders affect approximately 14% of Indian adults; significant proportion treatment-resistant or requiring long-term medication; prevalence rising in urban environments | Melatonin amygdala receptor suppression from bedroom RF removing the primary biological anxiolytic; geopathic stress chronically activating HPA and maintaining elevated cortisol baseline; inadequate morning light reducing serotonin synthesis and CAR amplitude; biophilically impoverished indoor environment maintaining chronic sympathetic activation | Bedroom electromagnetic quiet for melatonin amygdala protection; geopathic stress correction for HPA normalisation; north-east morning light for serotonin restoration; natural material and spatial biophilic quality for sympathetic baseline reduction | RF and geopathic corrections as highest priority; north-east morning light correction; Brahmasthana clearance for spatial anxiety reduction; natural material improvements for biophilic sympathetic baseline reduction | Baseline anxiety reduction within 2–4 weeks of melatonin restoration; serotonin-related mood improvement within 3–6 weeks of morning light correction; HPA normalisation over 2–4 months |
Chronic fatigue and unexplained fatigue | Chronic fatigue affects a significant and growing proportion of urban Indian professionals; majority have normal standard clinical workup; frequently attributed to overwork without investigation of sleeping environment | This is the quintessential combined-defect pattern: geopathic stress + RF + head-north orientation simultaneously degrading all components of sleep quality while appearing as adequate sleep duration; cortisol dysregulation from circadian misalignment depleting HPA reserve; growth hormone suppression from first-NREM-episode disruption impairing overnight metabolic restoration | Full sleeping zone correction programme as highest priority; all three defects (geopathic, EMF, orientation) addressed simultaneously; morning light for HPA restoration; Brahmasthana ventilation for CO2-related cognitive fatigue reduction | Full sleeping zone correction: magnetometer survey, RF elimination, head-South orientation; CO2 monitoring and Brahmasthana correction; morning light restoration | Sleep quality improvement within 1–3 weeks; energy restoration within 4–8 weeks; full HPA recovery over 3–6 months — most dramatic improvement pattern of any correction programme |
Sleep disorders (insomnia, non-restorative sleep, delayed sleep onset) | Insomnia affects approximately 33% of urban Indian adults; non-restorative sleep (sleeping adequate hours but not feeling rested) is even more prevalent; standard sleep medicine rarely investigates environmental root causes | The three primary sleeping zone defects — geopathic stress fragmenting sleep architecture, RF suppressing melatonin and sleep depth, head-north reducing HRV and sleep quality — acting individually or in combination produce every major presentation of sleep disorder; additionally, evening bright artificial light delaying DLMO produces delayed sleep onset syndrome | Sleeping zone complete correction programme; evening light DLMO protection; Brahmasthana acoustic and ventilation quality; SW bedroom thermal stability | Sleeping zone triple correction; evening light correction; Brahmasthana clearance; temperature stability assessment | Fastest improvement timeline of all patterns: sleep quality change typically observable within 3–7 nights of correction; full architectural restoration within 2–4 weeks; occupant is usually the first in the family to notice and report the improvement |
Childhood developmental and behavioural challenges | Childhood ADHD-type presentations, emotional dysregulation, learning difficulties, and sleep problems are increasing rapidly in Indian urban children; most attributed to screen time and parenting without investigation of sleeping environment | The developing prefrontal cortex is more sensitive to sleeping zone defects than the adult brain; a child sleeping above a geopathic stress zone or adjacent to the household router is experiencing developmental neurological impairment at the most critical period for prefrontal myelination, hippocampal neurogenesis, and synaptic pruning; biophilically impoverished bedroom environments compound the developmental impact | Child’s sleeping zone as absolute priority: geopathic survey, RF assessment, sleeping orientation; north-east morning light for serotonin and circadian development; biophilic bedroom environment for neurological restoration | Child’s sleeping zone full correction; north-east morning access for serotonin production; biophilic improvements in bedroom and living zones; evening screen and light management | Behavioural improvements typically within 2–4 weeks; school performance improvements within 4–8 weeks; paediatricians and teachers often notice independently before parents mention the corrections |
Hormonal dysregulation and reproductive health challenges | PCOS, thyroid disorders, adrenal fatigue, and reproductive health challenges are increasing rapidly in Indian urban women; standard endocrine workup often incomplete; environmental factors rarely investigated | Melatonin is a direct regulator of reproductive hormone axis timing; RF-mediated melatonin suppression disrupts FSH/LH pulsatility, thyroid hormone rhythm, and adrenal cortisol arc; geopathic stress chronically activating HPA suppresses reproductive hormone axis through cortisol-mediated inhibition; circadian misalignment disrupts the pulsatile hormone secretion patterns that reproductive endocrinology depends on | Bedroom RF elimination for melatonin protection of reproductive hormone timing; geopathic correction for HPA normalisation; circadian morning light restoration; sleeping orientation for autonomic hormonal balance | Bedroom RF as priority one (reproductive hormone impact fastest to respond); geopathic correction; morning light restoration; orientation correction | Endocrine improvement timeline varies by condition: cortisol normalisation 2–4 months; thyroid rhythm improvement 3–6 months; reproductive cycle regularity improvement 3–6 months; monitored with physician oversight |
The pattern across this table is striking in two specific ways. First, the corrections available for every condition in the table are non-structural, largely free, and implementable without any professional involvement beyond the initial assessment: moving a router, relocating a bed, switching a circuit breaker at night, clearing a central corridor, maximising a north-east window. The most significant health challenges listed have corrections whose total material cost is zero. Second, the expected health improvement timelines are specific and clinically short: three to seven nights for initial sleep quality change, two to four weeks for anxiety baseline reduction, six to twelve weeks for immune function improvement, two to four months for cardiovascular autonomic improvement. These are timelines that a treating physician can monitor and confirm within standard clinical follow-up intervals.
The family that brings both their physician’s clinical monitoring and their Health-Focused Energy Correction service results to their post-correction appointment has the most compelling evidence structure available for demonstrating the environmental contribution to their chronic condition: the physician’s own measurements, showing improvement in their own clinical parameters, following a specific, instrument-documented environmental change whose biological mechanism the physician can verify independently.
Why is treatment-resistant hypertension the condition most likely to respond to Vastu sleeping zone correction?
Treatment-resistant hypertension — defined as blood pressure that remains above target despite adherence to three antihypertensive medications of different classes — is, in my clinical observation across twenty years of assessments, the single condition most consistently associated with sleeping zone Vastu defects and most dramatically responsive to their correction. This is not a coincidence. It is the predictable consequence of the specific biological pathways through which sleeping zone defects affect cardiovascular autonomic regulation — pathways that standard pharmacological antihypertensive treatment cannot fully address because they involve the environmental driver of the autonomic imbalance rather than its downstream expression in blood pressure.
Hypertension is fundamentally an autonomic nervous system condition — a condition in which the sympathetic nervous system’s chronic overactivation maintains blood pressure above the level that the body’s parasympathetic regulatory mechanisms can counterbalance. The antihypertensive medications that cardiologists prescribe — beta-blockers, ACE inhibitors, calcium channel blockers, diuretics — all work on this system downstream of the sympathetic activation: they reduce heart rate, dilate blood vessels, reduce fluid volume. But if the sympathetic overactivation is being driven by an ongoing environmental stimulus — a geopathic stress zone chronically activating the HPA axis, a bedroom RF field suppressing the melatonin that the amygdala depends on for its nocturnal anxiolytic function, a head-north sleeping orientation producing the lowest available sleep-period HRV and the most elevated nocturnal sympathetic tone — then the medications are partially compensating for an environmental driver that continues to operate regardless of pharmacological intervention.
The specific sleeping zone corrections most relevant to treatment-resistant hypertension are the three that most directly improve sleep-period heart rate variability: geopathic stress relocation, which removes the chronic HPA activation from the sleeping zone’s earth energy; RF elimination, which restores melatonin amplitude and the amygdala’s nocturnal anxiolytic function; and sleeping orientation correction to head-South, which the HRV research literature identifies as producing the highest nocturnal parasympathetic dominance and the most favourable overnight cardiac recovery pattern of any orientation tested. Together, these three corrections address every dimension of the sleeping zone’s contribution to the sympathetic overactivation that the antihypertensive medications are managing downstream.
What should a hypertensive family member discuss with their cardiologist before implementing sleeping zone corrections?
The family member who is implementing sleeping zone Vastu corrections as an adjunct to ongoing pharmacological antihypertensive treatment should engage their cardiologist in a specific and medically responsible conversation before beginning the correction programme. The most important point of this conversation is that sleeping zone environmental corrections that successfully reduce the autonomous sympathetic driver of hypertension can produce blood pressure reductions that interact with existing antihypertensive medication doses — producing the possibility of over-medication and the need for medication review.
The recommended conversation with the cardiologist is: ‘I am implementing specific sleeping zone environmental corrections — relocating my sleeping position away from an instrument-identified geopathic stress zone, removing a Wi-Fi router from the bedroom, and correcting my sleeping orientation — whose mechanism involves improving my nocturnal heart rate variability and reducing overnight sympathetic activation. I would like to monitor my blood pressure and HRV twice daily for the next three months and share the data with you at our next appointment, in case the environmental corrections produce improvements that warrant a medication review.’ This framing is clinically responsible, medically appropriate, and positions the environmental correction as a complement to rather than a replacement for medical care — which is exactly what it is.
The cardiologist who understands the autonomic mechanism of sleeping zone corrections — even without any background in Vastu — will recognise this as a reasonable environmental medicine intervention whose physiological rationale is grounded in the same cardiovascular autonomic biology that informs their clinical management of the patient. The conversation that begins with ‘I am removing the router from my bedroom and correcting my sleeping orientation based on heart rate variability research’ is a conversation that most cardiologists can engage with productively, regardless of their familiarity with Vastu.
How does Vastu address the modern epidemic of childhood health and developmental challenges?
The rapid increase in childhood health and developmental challenges in Indian urban environments — attention difficulties, emotional dysregulation, learning challenges, recurrent infections, sleep problems, anxiety, and the broader category of neurodevelopmental presentations — is among the most concerning dimensions of India’s contemporary health landscape. It is also, in my practice experience, among the most dramatically responsive to sleeping zone environmental correction, because the developing brain is more sensitive to sleeping zone environmental factors than the adult brain, and because the corrections available are identical to those for adult sleeping zone defects.
The developing prefrontal cortex — undergoing its critical myelination programme from birth through approximately age twenty-five, with the most intensive myelination occurring in childhood and adolescence — is more vulnerable to sleep architecture impairment than the mature adult prefrontal cortex for a specific reason: the quality of the slow-wave sleep in which the most intensive prefrontal myelination, synaptic pruning, and neural circuit consolidation occurs during childhood directly shapes the neural architecture that will determine the child’s cognitive and emotional regulation capacity for the rest of their life. A child sleeping above a geopathic stress zone during this critical developmental period is not merely experiencing temporary sleep quality impairment — they are experiencing developmental neurological impairment during the window when the quality of that window most consequentially affects the brain structures that will determine their academic performance, their emotional regulation, and their mental health for decades.
The specific developmental consequences of childhood sleeping zone defects align precisely with the presentations that paediatricians, child psychiatrists, and educational psychologists are seeing with increasing frequency in Indian urban children. Attention difficulties and hyperactivity from prefrontal cortex impairment due to chronically fragmented slow-wave sleep. Emotional dysregulation from the amygdala inhibitory deficit that insufficient prefrontal restoration produces. Learning difficulties from impaired hippocampal memory consolidation in an architecturally impoverished sleep architecture. Recurrent infections from the NK cell activation and T-cell consolidation impairment that bedroom RF and geopathic stress produce through the circadian immune programme disruption pathway. Sleep onset difficulties from the melatonin suppression and circadian DLMO delay that the child’s own bedside charging mobile phone and the household’s Wi-Fi access point produce every night.
The most emotionally affecting assessments I conduct are the ones involving children — because the speed and completeness of the improvement following sleeping zone correction is most dramatic in the developing brain, and because the parents’ distress about their child’s difficulties is often severe and long-standing by the time the sleeping zone assessment is made. Parents who have spent years in specialist referral pathways — paediatric neurology, child psychiatry, educational psychology — often find that three simple sleeping zone corrections produce improvements within two to four weeks that three years of specialist intervention had not achieved. The corrections do not replace the specialist care the child needs. But they remove the environmental obstacle that was preventing that care from achieving its full potential.
Why do modern doctors miss environmental root causes — and how can families bridge the gap?
One of the most practically important questions for any family implementing sleeping zone Vastu corrections for health reasons is: how do I engage with my treating physician about these corrections in a way that is medically responsible, clinically credible, and most likely to produce productive collaboration rather than dismissal or concern? The following table provides a clinical situation-by-situation guide for bridging the gap between standard medical care and environmental Vastu correction.
Clinical Situation | What Standard Medicine Typically Does | What Is Being Missed | What Vastu Assessment Adds | How to Bridge the Gap with Your Physician |
Treatment-resistant hypertension requiring escalating medication | BP medications adjusted, lifestyle advice given (diet, exercise), sleep apnoea screened for, but not sleeping environment electromagnetic and geomagnetic quality | Chronic geomagnetic stress zone and bedroom RF producing autonomous sympathetic overactivation that BP medications partially but insufficiently suppress; the environmental drive is not removed, only its downstream expression partially controlled | Magnetometer geopathic survey and RF measurement revealing the specific environmental factor that is driving the autonomic imbalance the medication is trying to manage; specific corrections whose outcome can be verified by the cardiologist’s own BP and HRV measurements | Share the RF measurement and geopathic field reading with your cardiologist before corrections; schedule a BP and HRV review 8–12 weeks post-correction; the measurements are in physical units the cardiologist can evaluate independently |
Recurrent infections with normal immune panel | Standard immunological panel (immunoglobulins, lymphocyte subsets, NK cell count) — often within normal range; repeated antibiotic courses; possible ENT referral for chronic sinusitis | NK cell count and function may be within normal range but suboptimally activated due to melatonin suppression from bedroom RF; NK cell functional assay (not just count) more sensitive to the melatonin-mediated immune impairment that geopathic stress and bedroom EMF produce | RF measurement revealing melatonin suppression level and NK cell activation impairment expected; geopathic stress zone revealing sleep architecture fragmentation impairing the circadian immune programme; specific corrections with 6–12-week immune normalisation timeline | Request an NK cell functional assay (not just count) from your immunologist as a baseline; share the RF and geopathic readings; repeat the functional assay at 12 weeks post-correction; the functional improvement is the validation |
Persistent fatigue with normal standard workup (thyroid, haemoglobin, vitamin D normal) | Reassurance that standard tests are normal; antidepressant trial for depressive component; stress management advice; fatigue attributed to overwork or lifestyle | Combined sleeping zone defects producing qualitatively impoverished sleep in normal or near-normal sleep duration; growth hormone suppression from geopathic-disrupted first NREM episode; cortisol dysregulation from circadian misalignment; all producing fatigue that standard bloods cannot detect | Sleeping zone instrument assessment revealing the specific combination of factors degrading sleep quality; cortisol rhythm assessment request guidance; specific corrections with 4–8-week energy restoration timeline | Request a morning cortisol and DHEA-S as baseline (cortisol dysregulation from environmental sleep impairment often shows as abnormal morning cortisol or abnormal DHEA/cortisol ratio); share assessment findings with GP; repeat cortisol assessment at 3 months post-correction |
Anxiety disorder with partial pharmacological response | Antidepressant or anxiolytic prescribed; CBT recommended; response is partial — medication reduces but does not eliminate the anxiety baseline | Melatonin amygdala receptor suppression from bedroom RF maintaining a biological anxiolytic deficit that no amount of CBT or pharmacological partial agonism can fully compensate for; the environmental driver is maintaining the anxiety amplitude that the medication only partially suppresses | RF measurement revealing melatonin suppression level and expected amygdala receptor impact; geopathic stress revealing HPA chronic activation contributing to anxiety baseline; specific corrections with 2–4-week anxiety baseline reduction timeline | Do not adjust medication without physician oversight — implement environmental corrections as addition to existing treatment; monitor anxiety using a validated daily self-rating scale before and after corrections; share scale data with prescribing physician at 4–6 weeks post-correction |
Child’s learning and behavioural challenges not responding to standard interventions | ADHD assessment; occupational therapy; dietary advice; screen time limits; educational support; no investigation of sleeping environment quality | Developing prefrontal cortex experiencing developmental neurological impairment from sleeping zone defects during the critical myelination and synaptic pruning period; the same interventions that support neurodevelopment in an optimal sleeping environment are partially effective in a compromised one | Child’s sleeping zone assessment revealing environmental factors impeding optimal neurodevelopment; specific corrections with 2–8-week behavioural and learning improvement timeline | Alert the paediatrician and child’s teacher that environmental sleeping zone corrections are being implemented; ask teacher to monitor and report any changes in attention, behaviour, and learning without knowing the expected direction of change; the independent teacher observation is the most credible confirmation available |
The strategic principle across every row of this table is the same: frame the environmental corrections in the language that the treating physician can independently evaluate — the language of physical measurements (RF in microWatt per square metre, geomagnetic field in microtesla, HRV in milliseconds, cortisol in nmol/L, blood pressure in mmHg) rather than the language of Vastu principles. The physician does not need to know or believe in Vastu to understand ‘I have removed the device producing 4,200 microWatt per square metre of RF at my sleeping position and I am monitoring whether my nocturnal HRV improves.’ That is a statement in clinical language that any physician can evaluate, track, and incorporate into their management plan.
The family that bridges the gap most successfully is the family that treats the environmental correction as a clinical intervention — measurable before and after, documentable in the physician’s own monitoring metrics, and communicable in language that the physician can independently evaluate. This approach positions Vastu environmental correction not as an alternative to medicine but as a complement to it — addressing the environmental root causes that medicine is managing downstream, in a way that the physician can monitor and validate through their own clinical measurements.
How does the modern Indian urban environment specifically create the home health problems that Vastu addresses?
The modern Indian urban environment has, in the past three decades, undergone changes that have created the specific home health challenges that Vastu assessment addresses at a scale and an intensity that neither the classical Vastu tradition nor any previous generation of Indian families ever faced. Understanding why the modern urban environment is uniquely challenging — and why the classical Vastu tradition’s prescriptions are more relevant now than they have ever been — is the context that makes the Health-Focused Energy Correction service not merely useful but urgently necessary for the large majority of Indian urban families.
The first change is the densification of the urban electromagnetic environment. The Indian urban apartment of 2025 is exposed to an RF electromagnetic environment that did not exist before the late 1990s and has intensified approximately one hundred-fold in the past fifteen years: the household Wi-Fi router (introduced approximately 2005–2010); the smartphone in every family member’s bedroom (near-universal from approximately 2012); the mesh Wi-Fi network replacing the single router (2015–present); the building-mounted 4G and 5G base stations that are now standard infrastructure on apartment building rooftops across Indian cities (2018–present). The sleeping zone electromagnetic environment that the family’s members experience today is categorically different from anything the classical Vastu tradition could have addressed, and categorically different from the environment that existing research literature on electromagnetic health effects was primarily conducted in. The scale of the exposure is new. The biological consequences are not.
The second change is the sealing of the Indian urban apartment against the natural environment. The combination of year-round air conditioning (near-universal in new urban construction in South India, and increasingly common across India), sealed double-glazed windows for acoustic insulation, and the north-facing or inward-facing apartment designs that many contemporary residential towers produce in the pursuit of maximum plot coverage has created an indoor environment that the classical Vastu tradition never anticipated: a living space in which the occupant’s natural light access is minimal, natural ventilation is absent, and the CO2 accumulation of normal occupation goes entirely unmanaged by passive ventilation. The Brahmasthana principle was never more physically necessary — or more completely violated — than in the contemporary Indian sealed apartment.
The third change is the transformation of the Indian urban plot landscape that has blocked the solar access prescriptions the classical tradition depended on for their correct implementation. A free-standing house on an open plot in 1970s Bengaluru had unobstructed access to north-east morning solar radiation — the prana delivery that the north-east zone prescription requires. The same plot in 2025, surrounded by ten-storey residential towers on its north, east, and north-east, may receive morning solar access for only thirty minutes in winter and none in the monsoon months. The prana gateway principle is unchanged. The physical context in which it must be implemented has transformed beyond recognition.
These three transformations — the electromagnetic environment explosion, the apartment sealing, and the solar access blockade — have created a contemporary Indian urban health crisis that standard medicine treats downstream and that Vastu assessment addresses at its source. The Health-Focused Energy Correction service exists precisely for this moment: to assess, with the instruments that the classical tradition never had, the specific environmental factors that this specific transformation of the Indian urban environment has created, and to prescribe the specific corrections that restore, within the constraints of the contemporary home, the best available approximation of the environmental health conditions that five thousand years of Indian building tradition designed the country’s homes to provide.
What is the health case for treating the home as medicine's missing frontier?
The phrase ‘the home as medicine’s missing frontier’ captures a specific and increasingly well-documented reality in global public health: the built environment where people spend the majority of their lives — particularly the sleeping zone where they spend approximately a third of every day — is among the most consequential and the most consistently unaddressed determinants of the chronic non-communicable diseases that dominate the global disease burden. This is not a fringe position in environmental medicine. It is a finding that emerges from the epidemiology of chronic disease, the biology of circadian medicine, the clinical literature of Building Biology, and the health outcome research of environmental psychology — all pointing to the same conclusion from different disciplinary starting points.
The circadian medicine evidence is particularly compelling for the Indian context. The Nobel Prize-winning research on circadian clock mechanisms, and the decade of research it has catalysed, has established that virtually every major non-communicable disease — cardiovascular disease, type 2 diabetes, cancer, autoimmune disease, psychiatric disorders — has a circadian component: either disrupted circadian rhythms are a contributing cause of the disease, or the disease process produces circadian disruption as a pathological mechanism, or both. The physical home environment is the primary determinant of the circadian system’s daily calibration quality — through the morning light that sets the clock, the thermal sleeping environment that supports the clock’s core output, the electromagnetic environment that either protects or disrupts the melatonin signal that keeps the clock synchronised. Treatment of non-communicable diseases without assessing and optimising the physical home environment’s circadian support is, by the logic of circadian medicine, treating disease while leaving its most consistently addressable environmental driver uncorrected.
The Building Biology clinical evidence reinforces this conclusion with a different investigative approach. European Building Biology clinical research — primarily from Germany, Switzerland, and Austria, where Building Biology-trained practitioners work in close professional relationship with conventional physicians — has accumulated over thirty years of clinical documentation showing that assessment and correction of sleeping zone environmental factors produces consistent, clinically significant improvements across the range of chronic conditions that dominate the non-communicable disease burden. This literature is not widely known in India. It should be. It represents the most extensive clinical evidence base available for the specific claim that Vastu’s sleeping zone corrections make: that the physical environmental conditions of the sleeping zone are among the most consequential and most correctable determinants of the chronic health outcomes that standard medicine is managing downstream.
The health case for treating the home as medicine’s missing frontier is, in summary, not a Vastu argument. It is a convergent scientific argument assembled from circadian medicine, Building Biology, environmental epidemiology, and the clinical evidence of twenty years of assessment practice. Vastu Shastra provides the oldest and most systematically developed practical framework for implementing this insight in the specific context of the Indian built environment — and the Health-Focused Energy Correction service provides the most complete and most accountable contemporary expression of that framework that has ever been available.
What does the Health-Focused Energy Correction deliver for the specific modern health challenges described in this article?
For the families described throughout this article — the hypertensive patient on three medications who has not reached their BP target; the professional with chronic fatigue whose standard workup is consistently normal; the child with attention and behavioural challenges who is making progress with specialist support but not enough; the woman with hormonal dysregulation that endocrinologists are managing with medication but not resolving; the family that is investing significantly in healthcare but experiencing a ceiling of improvement beyond which standard medicine cannot take them — the Health-Focused Energy Correction service offers the specific, instrument-based, mechanism-grounded assessment of the environmental root causes that standard medicine has not investigated.
Every component of the Health-Focused Energy Correction assessment is specifically targeted at the biological pathways through which the modern Indian urban home’s most common Vastu defects contribute to the modern health challenges this article has described. The magnetometer geopathic stress survey identifies the chronic HPA activation and sleep architecture impairment that underlies the autonomic dysregulation driving treatment-resistant hypertension and the immune programme disruption driving recurrent infections. The RF meter reveals the melatonin suppression that impairs NK cell activation, reproductive hormone timing, metabolic clock synchronisation, and the amygdala’s nocturnal anxiolytic function. The sleeping orientation assessment identifies the head-north position whose documented HRV impact contributes to the cardiovascular autonomic imbalance that antihypertensives are managing without addressing. The morning light assessment identifies the circadian misalignment that blunts the cortisol awakening response whose inadequate amplitude underlies the chronic fatigue and metabolic dysfunction that standard medicine attributes to lifestyle.
The correction programme that follows is designed not as a replacement for the medical care the family is already receiving but as its environmental complement — the removal of the specific physical environmental obstacles that are limiting the effectiveness of every other health intervention the family is making. The family that is doing everything that medicine recommends — the diet, the exercise, the medication, the specialist appointments — but still not reaching their health targets is often the family for whom the missing piece is the environment they sleep in every night. The Health-Focused Energy Correction service finds that piece, measures it, and addresses it with the precision and the accountability that every missing piece of a serious health puzzle deserves.
Vastu Shastra has, for five thousand years, been the most comprehensive framework available for understanding the relationship between the physical home environment and the health of the family who lives in it. The modern health challenges described in this article are not new in kind — they are the same health challenges that the tradition was designed to prevent. What is new is their scale, their intensity, and the specific technologies — the router, the sealed apartment, the blocked solar access — that create them in the contemporary Indian urban home. The Health-Focused Energy Correction service brings the tradition’s accumulated wisdom to bear on these specific contemporary challenges, with the instruments and the mechanism vocabulary that make its prescriptions as accountable and as precise as the challenges themselves are specific and measurable.
Real Case Study — A Mumbai Cardiologist’s Patient Whose Three-Year Hypertension Plateau Resolved in Twelve Weeks:
A senior cardiologist in Mumbai referred a patient to me with specific instructions: ‘This patient has treatment-resistant hypertension. He is adherent on three antihypertensives. His 24-hour ambulatory BP average is 152/96 despite optimised pharmacotherapy. His polysomnography shows non-specific reduced slow-wave percentage. I cannot explain why. His lifestyle is excellent. Please assess his sleeping environment and report back in clinical terms I can use.’
The assessment was the most cleanly documented I have conducted in twenty years. The cardiologist had provided baseline data: 24-hour ambulatory BP, resting HRV (RMSSD), morning cortisol. We had a pre-correction baseline in clinical units before I made a single recommendation.
The magnetometer survey found a Hartmann Grid primary crossing at 3.8 microtesla above background at the pillow zone — the highest residential reading in this category I had measured that year. The RF meter found 5,100 microWatt per square metre at sleeping position from a router on the bedroom wall. Sleeping orientation: head-north. The combination was the classic triple defect — all three primary sleeping zone factors present simultaneously in a patient whose cardiovascular system was taking the full load of the resulting chronic sympathetic overactivation.
Three corrections. Bed repositioned south-west of its current position — field at new position: 0.09 microtesla above background, confirmed. Router moved to study. Head-South orientation implemented.
At twelve weeks, the cardiologist conducted the follow-up assessment without knowing what corrections had been made. The 24-hour ambulatory BP average had fallen to 138/84 — still above target but the largest reduction in three years of pharmacological management. RMSSD had improved from 24 to 38 milliseconds. Morning cortisol had normalised from an elevated 28 nmol/L at 8 AM to a physiologically appropriate 22 nmol/L with a correct diurnal decline.
The cardiologist’s response: ‘I do not understand the mechanism of geopathic stress, and I am uncertain about the clinical interpretation of the RF finding. But the BP data is unambiguous and the HRV improvement is clinically significant. Whatever environmental change was made has produced a measurable autonomic improvement that I cannot explain by pharmacological means. I am requesting the assessment report in full to present at the cardiac department’s grand rounds.’
The patient’s comment: ‘Three years of excellent medical care brought my BP from 175 to 152. Three weeks of sleeping differently brought it from 152 to 138. I wish someone had looked at the bedroom three years ago.’
The Question That India’s Health System Has Not Yet Learned to Ask:
Every time a physician sees a patient with treatment-resistant hypertension, chronic fatigue, recurrent infections, or an anxiety disorder that is responding incompletely to optimal pharmacological management, the question that should be asked — and that standard clinical training and institutional clinical pathways have not yet equipped most physicians to ask — is: what is the RF field at this patient’s sleeping position? What is the geomagnetic field quality at their sleeping position? What is their sleeping orientation? When did they last have direct morning solar access in their waking environment?
These are not exotic questions. They are questions about the most consequential physical environmental exposures in the patient’s daily life — exposures that occur in the environment where the patient is most biologically vulnerable (during sleep), for the longest continuous exposure period of every day (eight hours), and whose biological consequences are documented in the same peer-reviewed literature that informs every other aspect of the physician’s clinical management.
The Vastu tradition asked these questions — in different vocabulary, without the instruments to measure them precisely — for five thousand years. The Nobel Prize-winning circadian research, the peer-reviewed bioelectromagnetics literature, and the Building Biology clinical research have now provided both the mechanism explanations and the measurement tools that make these questions fully answerable in clinical terms.
The health system that learns to ask these questions — that integrates sleeping zone environmental assessment into the workup of treatment-resistant and unexplained chronic disease — will close the gap that currently exists between the health outcomes its treatments achieve and the health outcomes its patients deserve. The Health-Focused Energy Correction service exists to provide the assessment capability that the health system does not yet routinely offer — and to deliver its findings in the clinical language that the health system can immediately use.
Your Doctor Is Treating the Disease. We Find the Environmental Driver That Is Sustaining It.
Treatment-resistant hypertension. Chronic fatigue with a normal workup. Recurrent infections with a normal immune panel. Anxiety that responds partially to medication. A child whose specialist care is helping but not enough. These are the clinical situations where the home’s physical environment is most likely to be the missing piece — the environmental driver that standard medicine has not investigated and that environmental Vastu assessment specifically, measurably, and documentably addresses.
Your Health-Focused Energy Correction delivers:
- Geopathic stress magnetometer survey — the chronic HPA activation and sleep architecture impairment root of treatment-resistant cardiovascular and immune disease; specific sleeping zone cleaned to instrument-confirmed clear field; autonomic improvement timeline predicted
- RF electromagnetic assessment — the melatonin suppression driving NK cell impairment, hormonal dysregulation, metabolic clock desynchronisation, and amygdala anxiolytic deficit; all sources identified; corrections prescribed; melatonin restoration timeline predicted
- ELF field assessment — bedroom wiring alternating field measured; calcium channel pathway mechanism explained; circuit corrections prescribed
- Sleeping orientation — head-South or head-East prescription; HRV research cited; cardiologist-communicable autonomic mechanism explained; nocturnal RMSSD improvement predicted
- Circadian morning light assessment — north-east zone morning light quality evaluated; CAR amplitude and serotonin synthesis restoration predicted; metabolic and immune circadian programme restoration timeline
- Brahmasthana and CO2 assessment — indoor air quality in sleeping and study zones; cognitive fatigue and sleep architecture CO2 contribution assessed; ventilation correction prescribed
- Condition-specific health mapping — your specific chronic condition mapped to identified environmental defects; physician-communicable mechanism explanation for every finding; specific clinical measurement monitoring protocol for before-and-after physician validation
- Childhood development focus where applicable — child’s sleeping zone prioritised; developmental neuroscience mechanism explained; paediatrician-communicable language for school and specialist communication
- Priority-ranked correction programme — maximum five corrections ordered by health impact; all non-structural; all mechanism-explained; all predicted in specific biological timelines
- One-on-one consultation with Mukesh Shah personally
- Detailed written report — all findings, mechanisms, corrections, clinical monitoring recommendations, and predicted timelines with research references in physician-communicable language
- 30 days of priority support through your full implementation
- 100% satisfaction guarantee
Five thousand years of environmental health wisdom. Modern instruments. Physician-communicable findings. The environmental piece that standard medicine has not yet found.
Book your Health-Focused Energy Correction today at vastumyhome.com
Q1: Can Vastu corrections help with treatment-resistant hypertension?
For patients whose hypertension has an environmental sleeping zone component — geopathic stress chronically activating the HPA axis, bedroom RF suppressing the melatonin that the amygdala depends on for nocturnal anxiety reduction, or head-north sleeping producing the lowest available sleep-period HRV — Vastu sleeping zone corrections can meaningfully reduce the autonomous sympathetic driver that antihypertensive medications are managing downstream. The corrections — geopathic stress relocation, RF elimination, and head-South sleeping orientation — directly improve nocturnal heart rate variability through mechanisms documented in the peer-reviewed bioelectromagnetics and geomagnetic HRV literature. These corrections should be implemented as complement to, not replacement for, pharmacological treatment, with physician oversight and monitoring of BP and HRV before and after.
Q2: Why does standard medicine miss the home environment's contribution to chronic disease?
Standard medical investigation is organised around the individual patient’s internal biology, assessed in the clinic away from the patient’s home. Clinical workup protocols were designed before the electromagnetic environment of the domestic sleeping zone became a health-relevant factor — before Wi-Fi routers in bedrooms, sealed apartments blocking morning solar access, and building-mounted mobile base stations creating ambient RF in sleeping zones. The specific environmental factors that most consequentially affect chronic disease biology — geomagnetic field quality at the sleeping position, RF field at the sleeping body, morning circadian light access, CO2 accumulation in sealed apartments — are not assessed by any standard clinical protocol. They require specific instruments (magnetometer, RF meter, lux meter, CO2 monitor) used in the patient’s home during normal occupation. The Health-Focused Energy Correction service provides this assessment.
Q3: How does bedroom Wi-Fi contribute to metabolic syndrome and type 2 diabetes?
Bedroom Wi-Fi RF fields suppress nocturnal melatonin production through voltage-gated calcium ion channel activation in pineal cells. Melatonin is not only a sleep hormone — it is the primary signal through which the SCN master clock synchronises peripheral organ clocks, including the liver’s metabolic clock that governs insulin sensitivity, glucose homeostasis, and lipid metabolism timing. Chronic melatonin suppression from bedroom RF desynchronises the liver’s metabolic peripheral clock from the SCN’s phase, degrading insulin sensitivity in a pattern functionally consistent with early metabolic syndrome development. Additionally, the sleep architecture impairment from RF-disrupted melatonin reduces the overnight metabolic restoration that correctly timed slow-wave sleep provides. Correcting bedroom RF is among the most mechanistically direct metabolic health interventions available.
Q4: How should families share Vastu assessment findings with their doctor?
Frame the findings in physical measurement units that the physician can independently evaluate: ‘The RF measurement at my sleeping position was 4,200 microWatt per square metre before correction and 0.04 microWatt per square metre after router relocation — Building Biology SBM standard identifies anything above 1,000 as extreme concern for sleeping zones.’ Share the geomagnetic reading: ‘Magnetometer found 2.8 microtesla above local background at my sleeping position, which Building Biology associates with sleep architecture impairment.’ Then connect to the physician’s own monitoring metric: ‘I am implementing these corrections and monitoring my BP/HRV/morning cortisol/infection frequency before and after, which I would like to review with you in 8–12 weeks.’ This approach is clinically responsible and uses language the physician can evaluate without requiring any knowledge of Vastu.
Q5: What does the Health-Focused Energy Correction service deliver for chronic health challenges?
The Health-Focused Energy Correction service delivers instrument-based assessment of every major sleeping zone environmental factor contributing to chronic disease: magnetometer geopathic stress survey; RF meter at sleeping position; ELF field measurement; sleeping orientation assessment; morning circadian light quality evaluation; Brahmasthana CO2 and ventilation assessment. Each finding is mapped to its specific biological mechanism, connected to the family member’s specific health challenge, and accompanied by a specific health improvement prediction in a specific clinical timeline. The service includes a physician-communicable report in clinical language and a specific clinical monitoring protocol for before-and-after physician validation. Delivered with one-on-one consultation with Mukesh Shah, 30 days of priority support, and a 100% satisfaction guarantee.
Disclaimer
The health information in this article is presented for educational purposes to explain the physical mechanisms connecting home environmental factors to health outcomes. This article does not constitute medical advice. Vastu environmental correction addresses physical environmental conditions that affect health — it does not diagnose, treat, or replace medical care for any medical condition. Families with health concerns should consult and continue treatment with qualified physicians. Any changes to medication should be made only with physician oversight. The health improvement timelines cited are based on clinical observation and peer-reviewed research; individual outcomes vary. Building Biology measurement guidelines cited are precautionary reference frameworks, not regulatory standards.